thumb:
- pulleys: 2 annular pulleys and an oblique pulley (which arises from the aponeurosis of the adductor pollicis muscle (thenar eminence)
- tendons: flexor pollicis longus(fpl) runs through the carpal tunnel and thenar eminence to insert on the distal phalanx. flexor pollicis brevis forms the thenar eminence of the hand.

fingers:
- tendons: there are 2 primary flexor tendons of the 4 fingers:
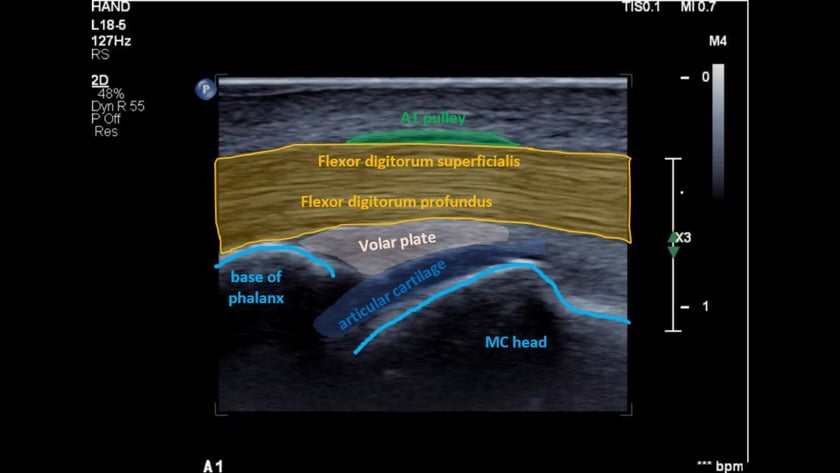
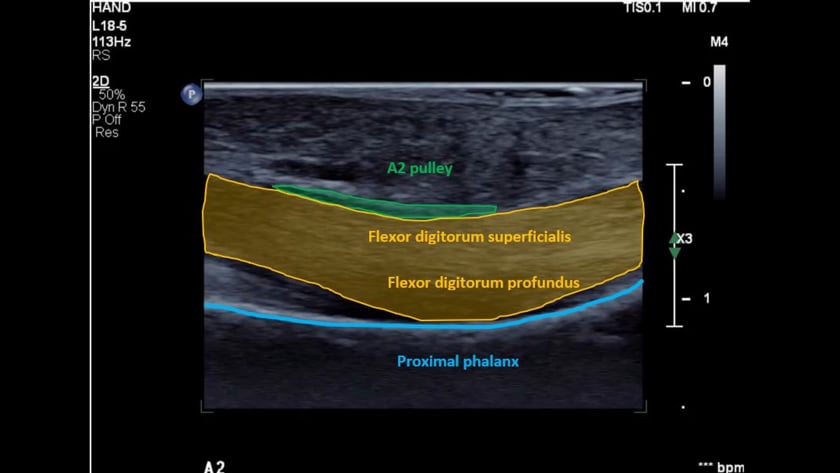
- flexor digitorum superficialis tendon(fds). this lies most superficial at the level of the metacarpal. it divides into 2 slips, each circling under the fdp tendon to insert as 2 separate slips onto the base of the middle phalanx. (function: flex the pipj)
- flexor digitorum profundus tendon (fdp) is deep to the fds. the fdp inserts onto the base of the distal phalanx. (function: flex the dipj)
- pulleys: role is to support and guide the flexor tendons along the bone.
5 annular pulleys (a1-5) and 3 cruciate pulleys (c1-3). the cruciate pulleys are poorly seen on ultrasound due to anisotrophy.
 |  |
to scan the hand and fingers:
- patient seated comfortably.
- on the edge of the bed with their hand on a pillow on their lap, or seated on a chair on the opposite side of the bed with their arm outstretched towards you.
- hand supported on a towel or similar.
tip: you will need the ability to flex/extend the fingers so ensure nothing obstructs this.
to examine the flexor tendons of the finger:
- place the transducer transversely across the palm of the hand just proximal to the base of the finger crease
- slide the probe distally in transverse following the tendons. fds to the base of the middle phalanx and fdp to the distal phalanx.
- rotate into longitudinal.
- confirm the distal fdp insertion.
- follow proximally in longitudinal to the palm.
- dynamically assess the tendons sliding. particularly under the a1 and a2 pulleys
- examine the insertions of the fds slips. from longitudinal over the midline of the base of the proximal phalanx, rotate the distal end of the probe slightly to the side so you are oblique. repeat for both radial and ulnar slips.
tips:
- at the proximal phalanx, fds will divide and rotate to be deep to the fdp.
- the tendon sheath begins approximately at the mid metacarpal and extends to the distal phalanx.
normal appearance of the flexor tendons:
- transverse: echogenic and ovoid
- longitudinal: echogenic and fibrillar.
- size: fds smaller than fdp
- no fluid should be visible.
- fds divides into 2 slips at the proximal phalanx. each slip equal in size and coursing around the side, then under the fdp.
- dynamics: the tendons should glide freely with finger flexion/extension.
tips:
- once at the level of the mid palm crease, it is common and normal to observe tendon bunching.
- once fds has divided, there will be anisotrophy of fds relative to fdp in the transverse plane. (ie one hypoechoic, when one is echogenic)
- fdp should sit against the proximal 1/3 of each phalanx. if not, suspect a pulley injury.
once you identify the flexor tendons of the finger:
- are they fibrillar and homogeneous?
- do the gradually decrease in size distally?
- there should be no fluid visible in the sheath.
- do they slide freely?
- is fdp against the proximal 1/3 of each phalanx?

thumb:
- tendons:
- extensor pollicis longus(epl) from compartment 3, inserts on the base of the distal phalanx.
- extensor pollicis brevis (epb) from the 1st wrist compatment to insert onto the base of the proximal phalanx.
- abductor pollicis longus (apl) also from the 1st wrist compartment. inserts on the base of the 1st metacarpal.

fingers:
- extensor tendons:
- extensor digitorum (ed).each of the 4 fingers has a single extensor digitorum tendon. from compartment 4 where it is the extensor communis and divides into 4 to insert on the base of each middle phalanx.
- extensor indicis (ei) is a 2nd extensor tendon to the index finger. it is also from compartment 4. at the level of the metacarpal head it joins with the ed tendon and also inserts on the base of the middle phalanx (slightly ulnar)
- extensor digiti minimi (edm) is a 2nd extensor tendon to the little finger. it is from compartment 5. at the level of the metacarpal head it joins with the ed tendon and also inserts on the base of the middle phalanx (slightly ulnar)
- extensor hood (eh):
- the extensor hood overlies the extensor digitorum with fascial anchoring bands on each side.
- at the level of the proximal interphalangeal joint it divides into 2 bands which rejoin for a common insertion on the base of the distal phalanx.

nailbed:
- the nail, nail bed (matrix) and underlying bone surface can easily be assessed.

a, nail plate; b, proximal nail (eponychial) fold; c, hyponychium; d, nail bed (sterile matrix); e, nail bed (germinal matrix); f, periosteum; g, bone of distal phalanx.
reproduced with permission from melanoma institute australia, copyright roula drossis
to scan the hand and fingers:
- patient seated comfortably.
- on the edge of the bed with their hand on a pillow on their lap, or seated on a chair on the opposite side of the bed with their arm outstretched towards you.
- hand supported on a towel or similar.
tip: you will need the ability to flex/extend the fingers so ensure nothing obstructs this.
to examine the extensor apparatus of the finger:
- place the transducer transversely across the distal metacarpal just proximal to the knuckle. the extensor should be directly beneath the probe.
- slide the probe distally in transverse following the extensor digitorum to the base of the middle phalanx.
- rotate into longitudinal.
- confirm the ed insertion.
- now move distally to confirm the extensor hood insertion to the distal phalanx.
- to assess each band of the extensor hood, keep the distal end of the probe on the insertion and rotate the proximal end very slightly to the radial, then ulnar aspects.
- dynamically assess the ed tendon sliding. at the level of the metacarpal head. importantly both in longitudinal and transverse (checking for tendon stability).
tips:
- if you see a nice round ed tendon, it is probably abnormally thickened.
to examine the nail bed of the finger:
- place the transducer (++gel) longitudinally on the finger nail.
- ensure you can see the nail root proximally.
- slide sideways assessing the entire area.
- rotate into transverse and assess proximaly-distally.
- carefully check the underlying bony cortex for defects.
- check with colour doppler.
tips:
- if you are uncertain, check neighbouring fingers.
normal appearance of the extensor tendons:
- transverse: echogenic and flat ovoid
- longitudinal: echogenic and fibrillar.
- size: <2mm
- no fluid should be visible.
- dynamics: the extensor tendon should glide freely and with stability at the level of the mcpj with finger flexion/extension.
normal appearance of the extensor hood:
- in the normal patient it cannot be seen independant of the extensor digitorum tendon.
- each band over the middle phallanx should be thin, parallel echogenic lines, shlightly hypoechoic centrally (with current technology)
- at the distal insertion it should be tapering, uniform, echogenic and fibrillar.
normal appearance of the nail bed:
- smooth underlying cortex
- hypoechoic nail matrix
- smooth, uniform parallel surfaces of the nail.
- the nail should taper evenly to a sharp nail root.
- uniform vascularity of the nail matrix with colour doppler.
once you identify the extensor apparatus of the finger:
- are they fibrillar and homogeneous?
- do the gradually decrease in size distally?
- there should be no fluid visible.
- do they slide freely?
- does the ed stay in place at the metacarpal head during finger flexion (transverse plane is best). if the ed subluxes, there is a likely tear of the sagittal band of the extensor hood.
- are both bands of the distal extensor hood intact 9partial mallet finger)
once you identify the nail bed of the finger:
- is it uniform in thickness?
- is there any underlying bony irregularity/defect?
- is there a mass/collection?
- is there focal hyperaemia on colour doppler?