

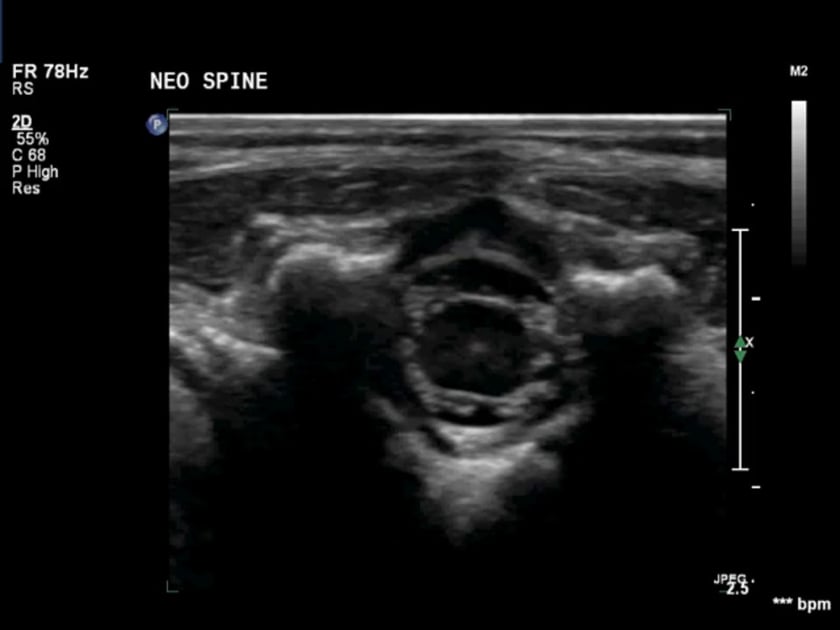
ultrasound neonatal spine ts superior to conus
transverse ultrasound cephalad to conus showing the nerve roots around the normal spinal cord.
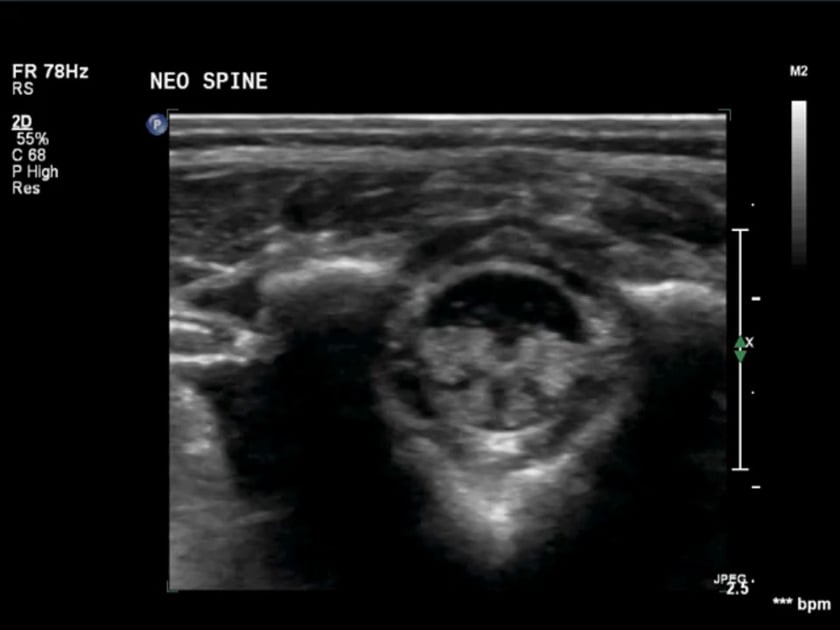
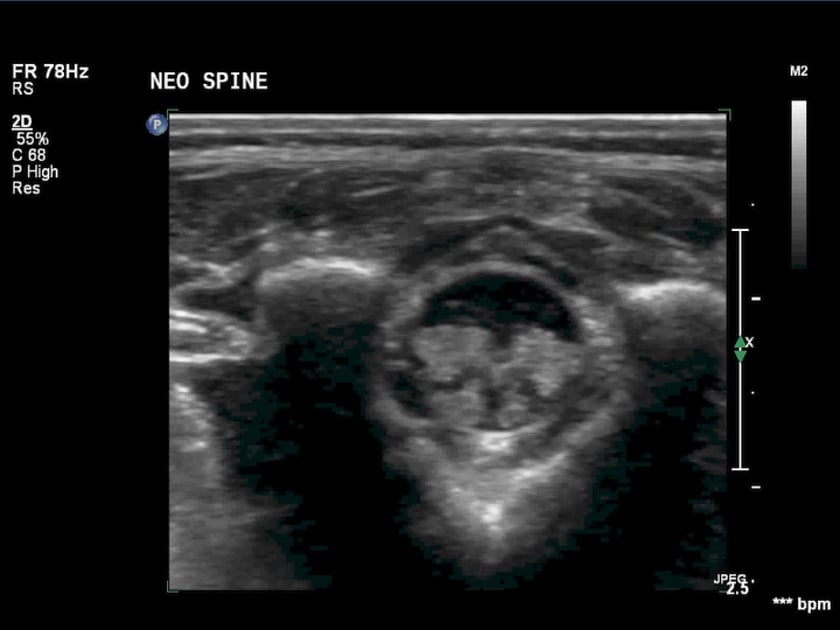
ultrasound neonatal spine ts at conus
transverse ultrasound of normal neonatal spine at the tip of conus showing the normal nerve root oscillations.
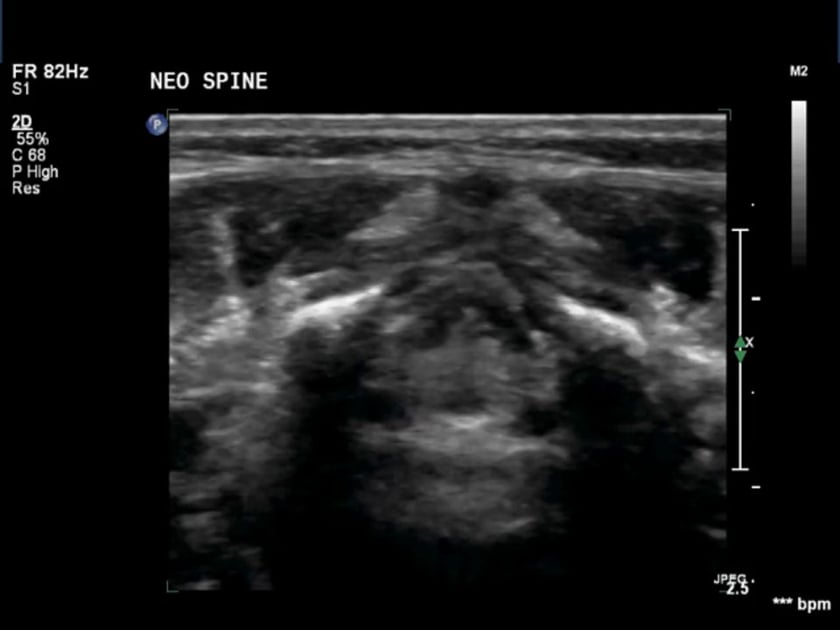
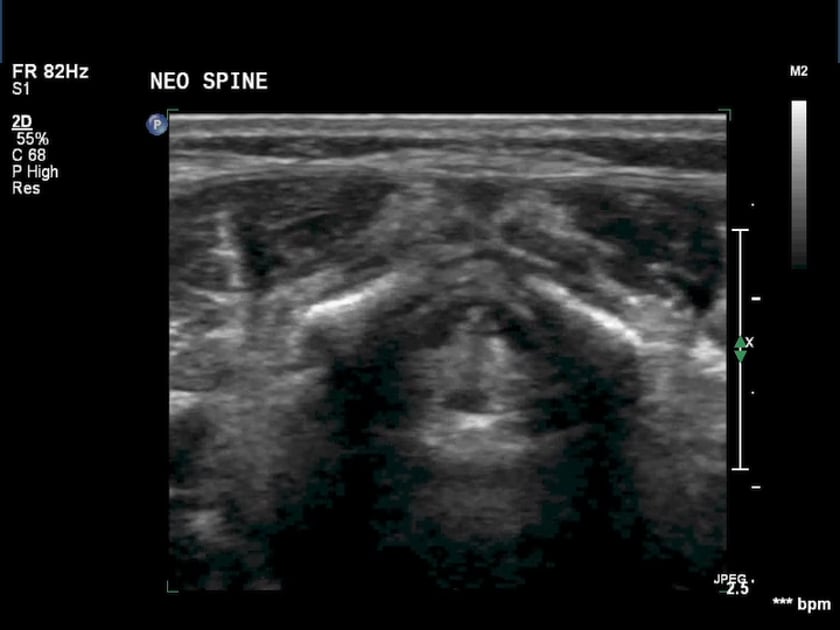
ultrasound neonatal spine ts inferior to conus
transverse ultrasound view of the inferior normal neonatal spine. note the normal cardiac and respiratory oscillation of the nerve roots.
ultrasound neonatal spine ls at conus
sagittal ultrasound of the neonatal spine at conus showing , filum and the normal nerve roots.
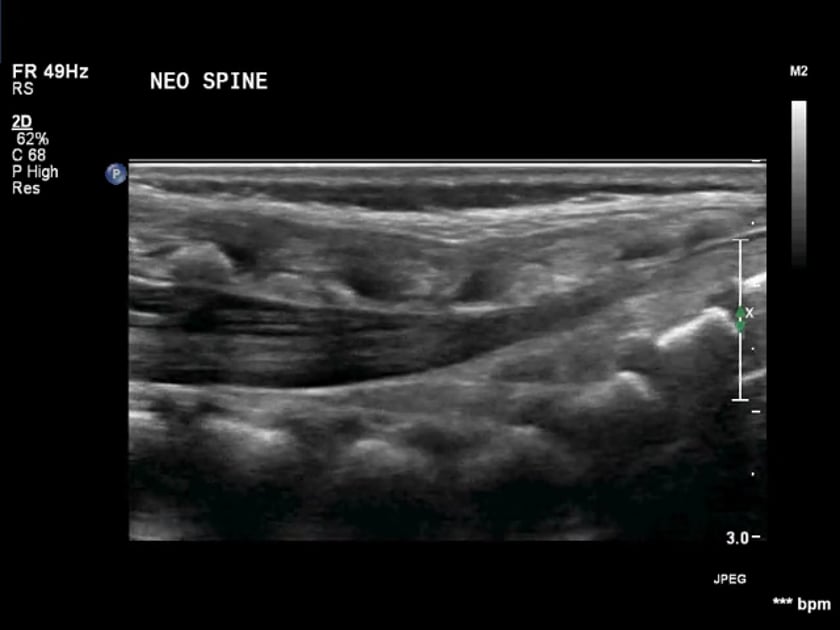
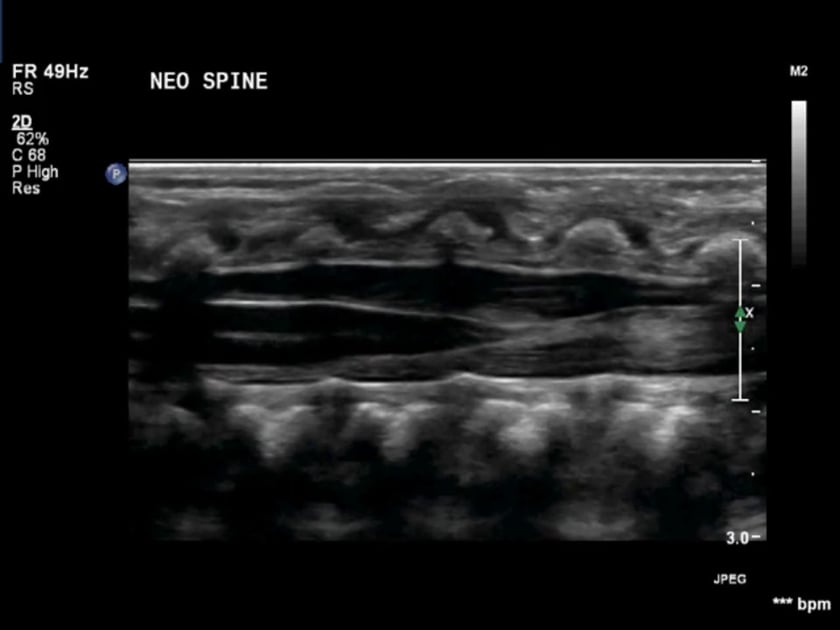
neonatal spine ultrasound normal sagittal
longitudinal ultrasound of the neonatal spine from the sacrum up to the lower thoracic region. the nerve rooots and filum are seen converging towards conus medullaris and then along the cord.
ultrasound neonatal spine normal conus
transverse ultrasound at the tip of conus medullaris. filum terminale can be seen centrally between the cauda equina bundles.
ultrasound neonatal spine normal inferior
the normal oscillations of the nerve roots of cauda equina in the dependant aspect of the thecal sac