
trochanteric bursa movement ultrasound
ultrasound of a normal trochanteric bursa. this demonstrates the best method to mobilise the anatomy and identify the trochanteric bursa.
knees together. gently raise the top foot.
the itb will be seen sliding over the gluteal tendons (or on the bone if the gluteals are torn). the thin hypoechoic layer under the itb is the trochanteric bursa.

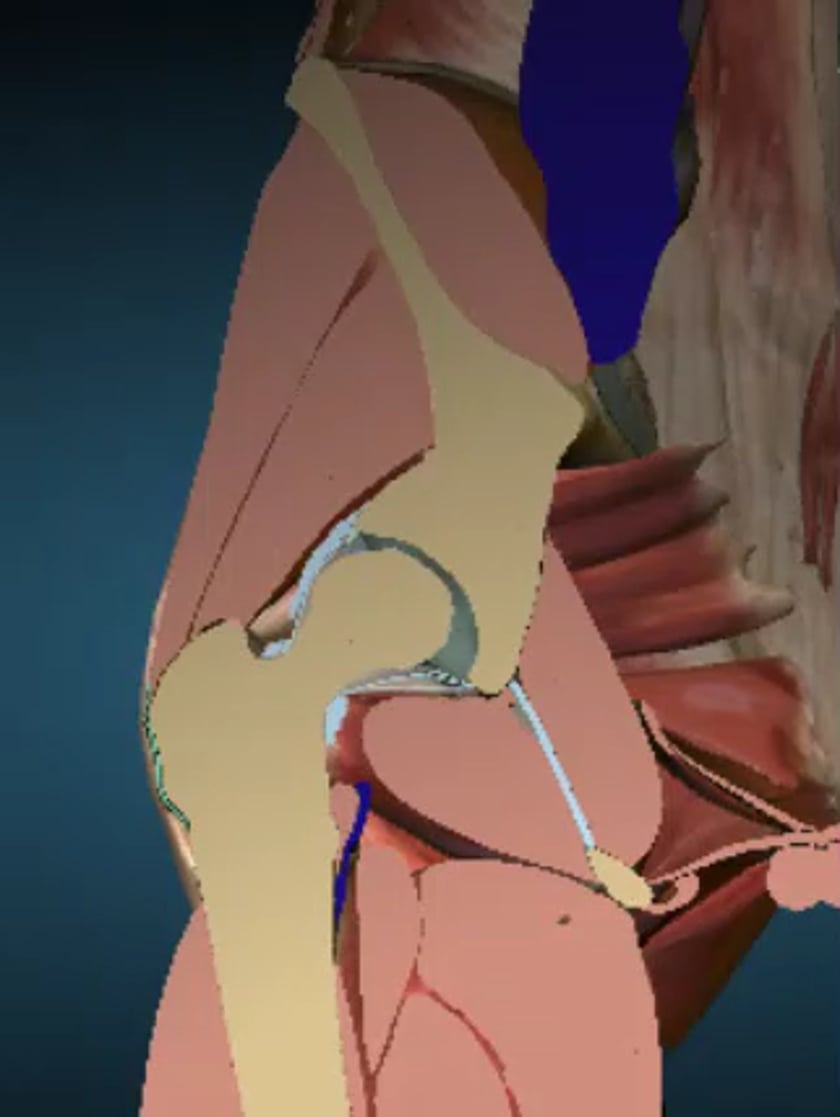
rectus femoris origin
the rectus femoris origin at the anterior inferior iliac spine (aiis)
anatomy
iliopsoas muscle and sartorius

origin of semimembranosus attachment
it is deep to the semitendinosis tendon on the ischial tuberosity.