

fetal circulation
by lisa mccabe, for openpediatrics
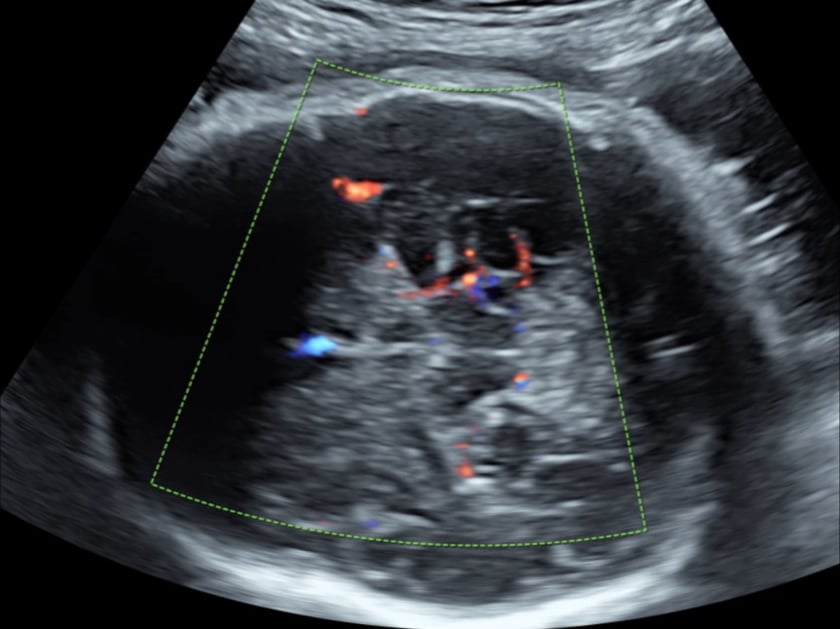
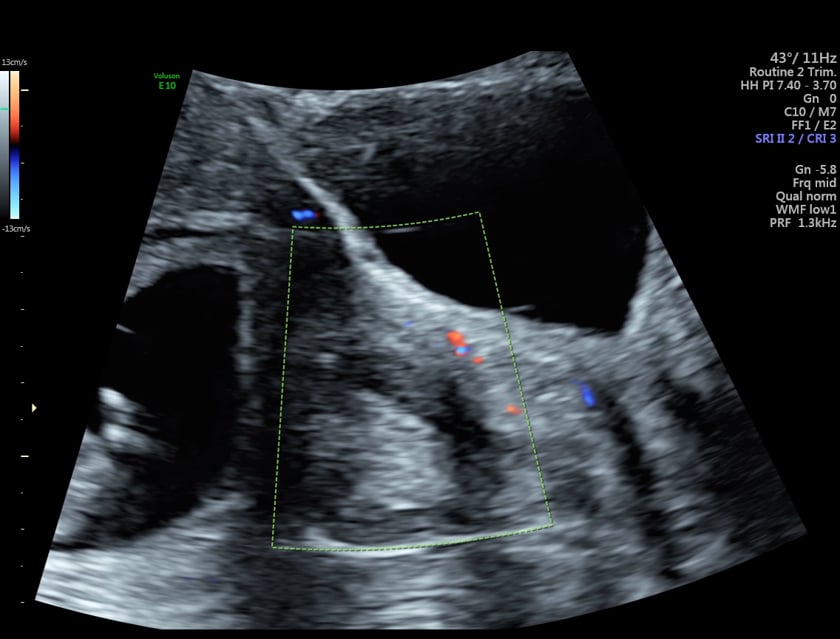
mca colour doppler ultrasound
evaluating the mca with colour doppler ultrasound. using the parietal bone as an acoustic window avoids shadowing from the petrous temporal bones or frontal suture.
mca doppler - with sound
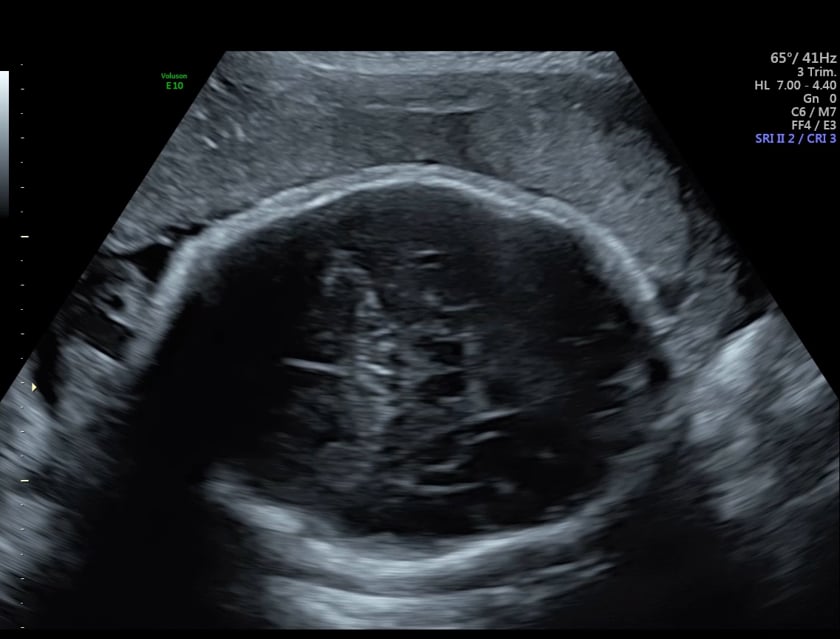
middle cerebral artery doppler 3rd trimester obstetric ultrasound
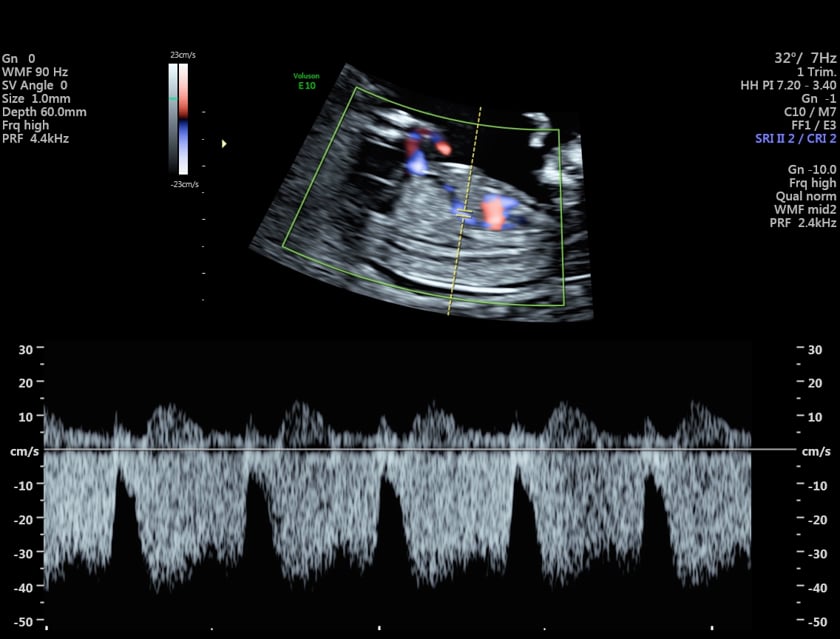
ductus venosus doppler - 1st trimester
a parasagittal plane. the normal dv flow is displayed below the baseline in this example. higher resistance (end diastolic flow approaching the baseline).
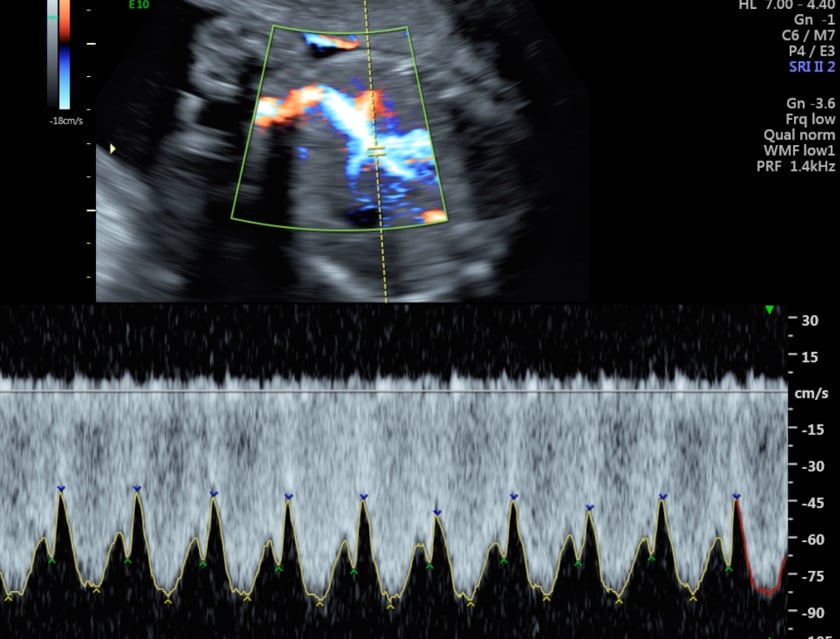
ductus venosus doppler - 3rd trimester
3rd trimester axial plane.
the normal lower resistance waveform of ductus venosus in the 3rd trimester.
ultrasound uterine artery doppler at 12 weeks gestation
with sound. approach is lateral to the cervix.

uterine artery doppler at 19weeks with sound
the uterine artery sampled adjacent to the external iliac artery. normal low resistance flow.