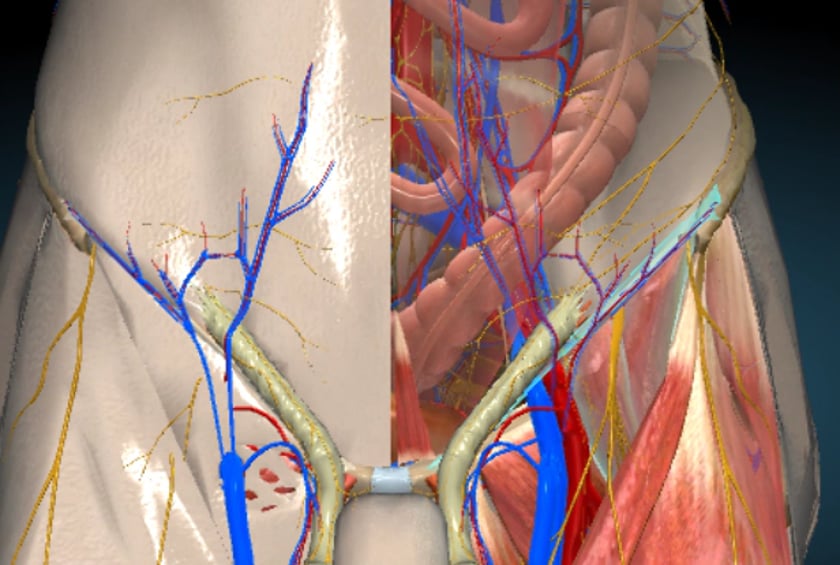
the femoral canal is bordered by the inguinal ligament antero-superiorly, posteriorly by the pectineal ligament, laterally by the femoral vein and medially by the lacunar ligament.
the bowel can herniate at the femoral ring thus called a femoral hernia.
anatomy
the inguinal ligament is seen crossing over the femoral vessels.
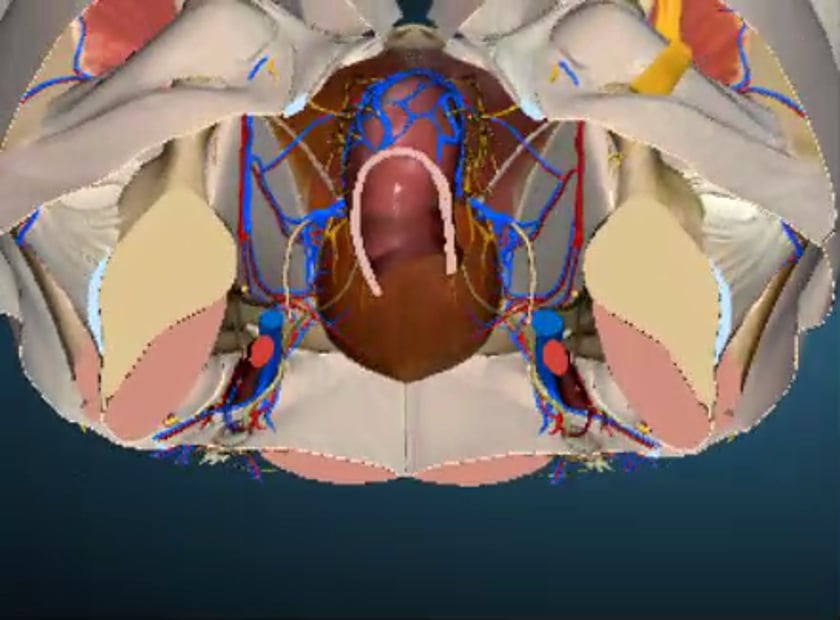
the femoral ring can increase in size if bowel or omentum moves into this canal.
femoral canal
the femoral canal can be appreciated above with the inguinal ligament (light blue) anteriorly positioned over the femoral vessels. the small space should only allow the nerve and vessels to course through this space.
femoral canal
transverse view of a femoral hernia. note that it descends medial to the common femoral vein.
ultrasound of the right femoral canal in transverse. the mouse over shows the expanding common femoral vein with the valsalva manouevre. the femoral canal is medial to the vessels. the vein would be compressed by the hernia and no dilatation would be observed.
inguinal canal
inguinal canal anatomy
it is important to understand the anatomy in order to decide if the hernia is direct or indirect.
the labelled anatomy is appreciated in the video.
inguinal canal
epigastric vessels are appreciated medial to the internal inguinal ring and the femoral vessels are inferior.
inguinal hernias
direct inguinal hernia
direct hernia.
ultrasound of direct hernia is seen medial to the inferior epigastric vessels
indirect inguinal hernia
indirect hernia
to image an indirect hernia start from down at the common femoral vessels and work your way in a transverse plane superiorly until you reach the level above where the inferior epigastric vessels join the ext iliac vein and artery.
longitudinal ultrasound of the normal spermatic cord at the internal inguinal ring. prominent vessels are commonly seen.
scan protocol
role of ultrasound
ultrasound is a valuable diagnostic tool in assessing the following indications;
muscular, tendinous and some ligamentous damage (chronic and acute)
bursitis
joint effusion
vascular pathology
haematomas
soft tissue masses such as ganglia, lipomas
classification of a mass eg solid, cystic, mixed
post surgical complications eg abscess, oedema
guidance of injection, aspiration or biopsy
some boney pathology.
limitations
the size of the patient can limit the visualisation of the normal anatomical landmarks.
patient preparation
before scanning know the origins and insertion sites of the gluteus minimus, gluteus medius, gluteus maximus, piriformis tendons and the fascia latae position
know the 3 common sites of bursitis
roll patient onto unaffected side initially then assess supine and compare
start with a curved linear array probe approx 6-8mhz to assess the muscles deep to the hip
to evaluate the bursae use a 7-12mhz linear probe
use a multi focus
narrow the dynamic range
ask the patient where the pain is and scan there first
run the probe up and down the lateral hip aligned to the long axis of the femoral shaft, and then move anterior and posterior
look in coronal and transverse
compare sides
remember that fluid is mobile and gravity dependant so do not over compress and do look in supine .also vary the patients leg position from extension to flexion and even abduction if this creates the pain.look at the patient erect.
equipment setup
use of a high resolution probe (7-15mhz) is essential.
careful scanning technique to avoid anisotropy (and possible misdiagnosis).
beam steering or compounding can help to overcome anisotropy in linear structures such as tendons.
good colour / power / doppler capabilities when assessing vessels or vascularity of a structure.
be prepared to change frequency output of probe (or probes) to adequately assess both superficial and deeper structures.